Atropine: Structure Activity Relationship
Today we will explore the structure activity relationship of atropine. Definitely more chemistry here, please revise the previous two articles before continuing.
 |
| Datura innoxia |
Previously,
we learnt that atropine is a tropane alkaloid which is an ester of tropanol
alcohol and tropic acid. It acts on the muscarinic acetylcholine receptors
(mAChRs) found in the central nervous system, as well as parasympathetic division
of the peripheral nervous system. The mAChR is a G-protein coupled receptor which relies on secondary messengers to elicit its action. To be precise,
atropine is a reversible competitive antagonist of mAChR. This means
that atropine readily competes with the natural (endogenous) neurotransmitter acetylcholine
and prevents it from activating mAChRs. In analogy, atropine is a naughty
kid who sticks the wrong key into your door every time you wish to
unlock it. Given enough naughty
kids, you may not be able to unlock your door anymore!
On a
molecular level, receptor antagonist binds to the same receptor as endogenous neurotransmitter, but it does not elicit any response. Given atropine and acetylcholine together, atropine of increasing concentration will diminish and
eventually abolish the innate activity of acetylcholine. However, if we increase the concentration of acetylcholine, it
will displace atropine from mAChR, which resumes action. This is called reversible competitive antagonism. On a
biological level, the antagonism of mAChR will diminish parasympathetic control. This causes the sympathetic division to go into overdrive, giving the impression that atropine does the opposite of acetylcholine.
Think about it this way, atropine deactivates the decelerate paddle of a car,
this disables the car to slow down. It gradually accelerates out
of control, but atropine never affects the accelerate paddle.
That
said, atropine must bind to mAChRs, but unlike ACh,
atropine induces a different structural change such that mAChR does not become activated (no downstream signaling, no second messenger). That means
the two chemical molecules are very similar, but not entirely so. Atropine has to do whatever acetylcholine does in receptor binding, but it has extra
chemical substituents. Recall that drug-receptor binding
isn’t caused by chemical reaction, instead attraction of certain atoms to one another. These are inter-molecular
attractions and they may or may not be permanent. The
latter applies to ACh and atropine, hence their reversible effects. If drug
binding is not reversible, the outcome can be disastrous.
There are a few
types of inter-molecular attractions which are relevant to us. First, there is electrostatic
attraction of positively charged atom to negatively charged atom (+ ---
-). Secondly, hydrogen-bonding like those in water (H2O---H2O) bonds H to O, N and F atoms. Thirdly, atoms or molecules can attract each other between
regions of poor and rich electron density (dipole), a force called Van Der
Waals attraction. Finally, there is pi-stacking attraction, where aromatic
rings tend to attract each other.
Pharmacologists study the structure activity relationship (SAR) of a drug by removing
or adding different chemical substituents, then comparing the biological effect with endogenous neurotransmitter or drug standards. Chemical structures which are crucial to receptor binding and activity can therefore be deduced. The advent of physics allows scientists to crystalise proteins including mAChRs
together with a drug, and then solve the entire structure using X-ray (X-ray
crystallography). This enables visualisation the inter-molecular attraction within drug-receptor complex. Super
computers are also employed to
calculate and model different shapes of drugs-receptor complexes. Understanding of SAR is vital to the development of more effective and safer drugs.
 |
Figure 1: Structure activity relationship of atropine in relation to MAChR. |
Examine Figure 1 carefully, it shows the SAR of ACh and
atropine. Notice that both of ACh and atropine are esters (blue). They also have
a nitrogen atom (red), and two or three carbon atoms that bridge the
nitrogen to ester group (red bolded bonds). In human body, the
nitrogen atom of atropine behaves as an
alkali, it will react with acids to produce a positively charged ion,
called ammonium (NH+). ACh on the other hand carries a permanent
positive charge on its nitrogen atom called trimethylammonium (NMe3+).
Atropine also has additional aromatic ring and a branched alcohol (OH
group) in its tropic acid component. Knowing
these, we can deduce the binding requirements of mAChR. First, there is electrostatic attraction between
the positive ammonium to
negatively charged protein (NH+ ------ -OOC). Two or three
carbon bonds away, there is hydrogen bonding between ester (carbonyl oxygen) of atropine and ACh with amino-hydrogen atoms of mAChR (NH2 ---- O-C=O---- H2N). The two to three carbon distance is crucial because any shorter or longer would not allow inter-molecular attraction. Similarly, if there is
no positive charge on nitrogen atom, or a lack of an ester (carbonyl) group, mAChR binding would fail. In fact, the binding pockets of mAChR is a 'tight-fit' because ACh itself is a small molecule.
Unlike ACh, atropine has an aromatic ring and branched alcohol in its tropic acid fragment. These confer huge
antagonistic activity, hence inferring extra inter-molecular interactions with mAChR. First, there is pi-stacking interaction between
the aromatic ring of atropine with aromatic amino acids located below the ACh
binding site of mAChR. Secondly, hydrogen bonding occurs between branched OH
group with carbonyl groups of amino acids. The extra intermolecular attractions induce a different conformational change such that mAChR is not activated. Remember that intermolecular interactions are not
permanent? Given enough time, both atropine and ACh will dissociate
(unbound) from mAChR all on their own. That’s why they can compete with each
other. Nonetheless, atropine and scopolamine have high affinity to mAChR, they are very potent. The two still remain as gold standard
anti-muscarinic agents.
Knowing
the SAR of atropine allows us to do more. We can alter the structure of
atropine, even removing the tropane ring all together, but still develop
analogs which are anti-muscarinic. We can make analogs with
permanently positive nitrogen atom, which do not cross the blood-brain
barrier. This reduces central nervous system side effects like sedation and delirium. Many anti-muscarinic drugs are used in modern medicine to treat motion sickness, reduce
secretions and urinary incontinence, dilate pupils for examination (mydriatic),
alleviate asthma by dilating airway, inhibit spasm, and control the symptoms of
Parkinson’s disease. Atropine
is used to speed the heart in an event of abnormally low heart rate (bradycardia, medical emergency). It
is also used to counteract the cholinergic effects of neostigmine, a paralytic agent commonly used in general anaesthesia. Similarly, atropine is an antidote
to pesticides or even nerve gas poisoning, which causes sympathetic crisis. The toxic effects of an agonist (nerve gas) and antagonist (atropine)
cancel out each other!
The infamous scopolamine, AKA the
‘Devil’s breath’ is reportedly used as truth serum to extract information out
of people and then have their memories ‘erased’. I remain skeptical of these
accounts, but there is a grain of truth. Scopolamine is an oily liquid, its salts are hygroscopic solids (readily absorbs moisture from air). The pure drug cannot be blown into people's face as a power, it probably has to be adsorbed onto some inert material to achieve devious goals. On a brighter
side, scopolamine is used as transdermal patch placed behind the ear to treat motion sickness. Figure 2 lists some common anti-muscarinic drugs used in modern medicine, you can examine their structures to determine the
SAR of atropine. Remarkably, there is an ultra-potent, but less toxic analog
of atropine called 3-quinuclidinyl benzilate, which was developed by the US
military (designated as agent BZ) as a psychosomatic chemical weapon! It is aimed to
incapacitate a lot of people via anticholinergic toxidrome. Luckily, BZ is
outlawed by the chemical weapons convention, let’s hope it stays
that way.
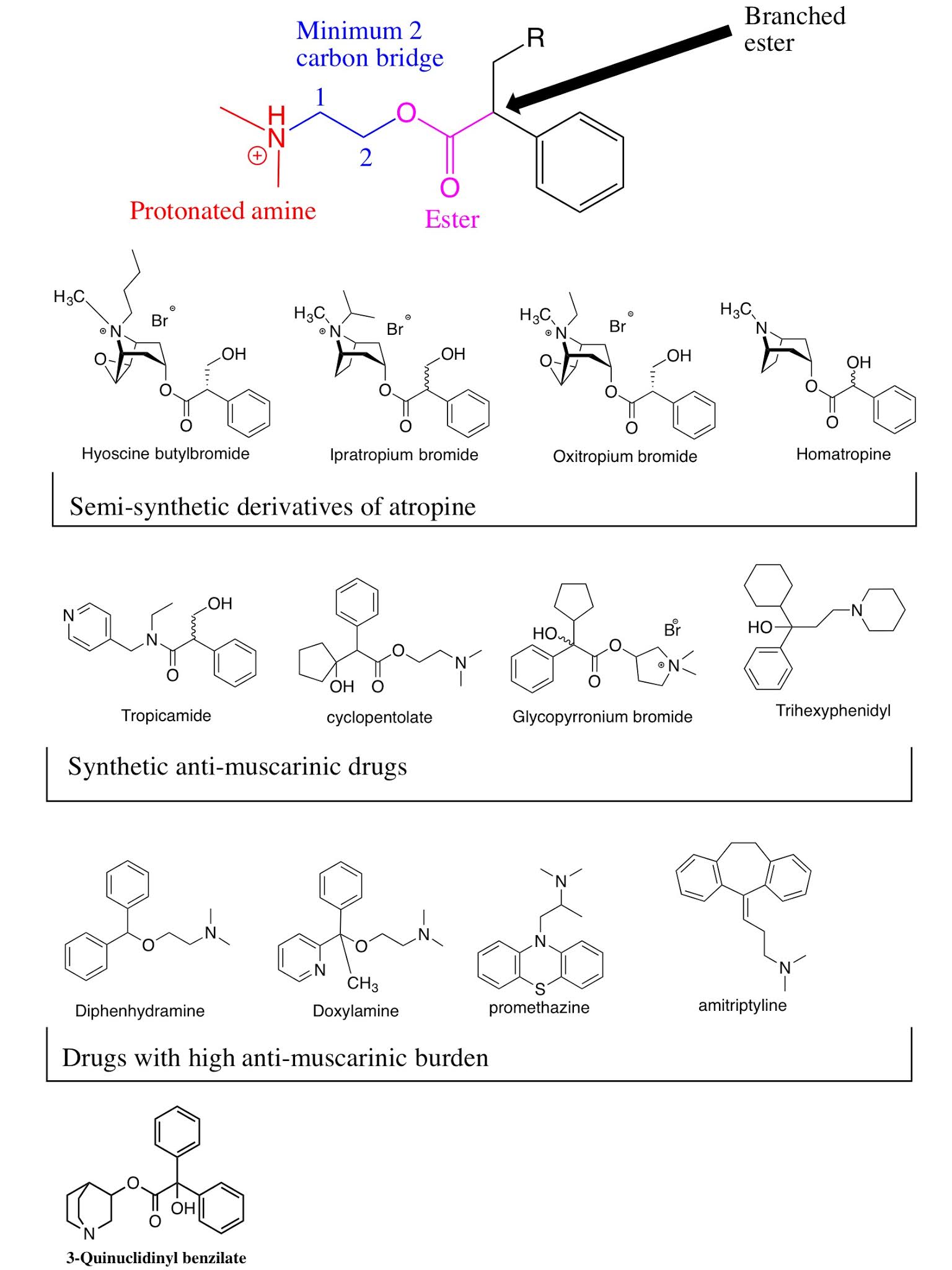 |
Figure 2: Examples of antimuscarinic drugs. |
Finally, here's the answer to last week's homework. The M of muscarinic
acetylcholine receptor stands for muscarine. Muscarine is an alkaloid toxin which is isolated from hallucinogenic mushrooms such as Amanita muscaria. It activates mAChR so effectively (agonist), scientists named the receptor after muscarine (similar to nicotine and nAChR)! Examine the
structure of muscarine in Figure 1 and compare it to the SAR of ACh, you’ll
get better answer.
Here's something interesting, perhaps enforced by urban legends and movies. When a patient is about to die,
doctors can give shots which ‘strengthen’ the heart and prevent death-rattle, enabling final words and farewell. That’s likely atropine! What an
epiphany, atropine…Atropos… Cut the thread of life? In our journey to
understand this most canonical poison, we have seen how humans have
transformed poison into medicine, herbs into pills and superstition into
science.


Comments
Post a Comment